While deploying old-school Palm Pilots during a psychopathology research project, Dror Ben-Zeev, PhD made a surprising discovery. The device had elicited an unintended outcome—it helped study participants feel better.
“At the time we thought this was bizarre,” he says. “We weren’t intending to use the device to help them, we were using it as a clinical assessment tool to collect information about how they were feeling and how they were doing, which they recorded on the Palm Pilot.”

Comments culled from the clinical samples such as, ‘Thanks, that really helped me,’ made it clear that even though participants knew they weren’t interacting with another person, they felt better by the end of the study. “Drawing their attention to their illness and engaging them in introspection multiple times a day gave them the sense that someone was interested in them and supportive,” Ben-Zeev recalls. “We were asking questions but not in real time and they knew that,” he adds. “But they still thought it was helpful.”
The idea of using a mobile device to treat patients with mental health issues captured Ben-Zeev’s imagination and he wondered: What would happen if we created a treatment model using mobile technology?
Flash forward a few years and Ben-Zeev, an assistant professor of psychiatry at Dartmouth’s Geisel School of Medicine, is at the forefront of developing mobile health (mHealth) interventions for people with serious mental illness. His work focuses on the complex challenge of integrating effective health technologies into traditional systems of health care, developing psychosocial interventions for psychosis, and testing those applications for efficacy.
He first developed basic text message self-management interventions for schizophrenia patients, which eventually led to the creation of FOCUS, a sophisticated smartphone system designed to help individuals manage their illness. Schizophrenia is an illness that causes severe mental disturbances that disrupt normal thought, speech, and behavior. Symptoms include delusions, thought disorders, and hallucinations—people may hear voices, believe others are reading their minds, controlling their thoughts, or plotting to harm them, and also have difficulties in achieving goals.
“The idea is that you now have therapeutic reach that extends beyond a physical clinic and may be used in a way that face-to-face interaction can’t,” he says.
It’s true that the first route of intervention for people with psychosis is anti-psychotic medication, Ben-Zeev says, but many either don’t adhere to their medications or don’t benefit from them, and a lot of people don’t want to take medications. “The reason we are using smartphones, is that you don’t have to wait until your once-a-week or once-a-month psychotherapeutic session,” he explains. “Once downloaded, you can use the app’s tools to address some of your problems wherever and whenever you choose. If you are struggling with auditory hallucinations, which can happen at any time, you can get the support you need even if you are waiting at a bus stop,” Ben-Zeev adds. Mobile phone use among people with severe psychiatric disabilities is not that different from the general population, he notes.
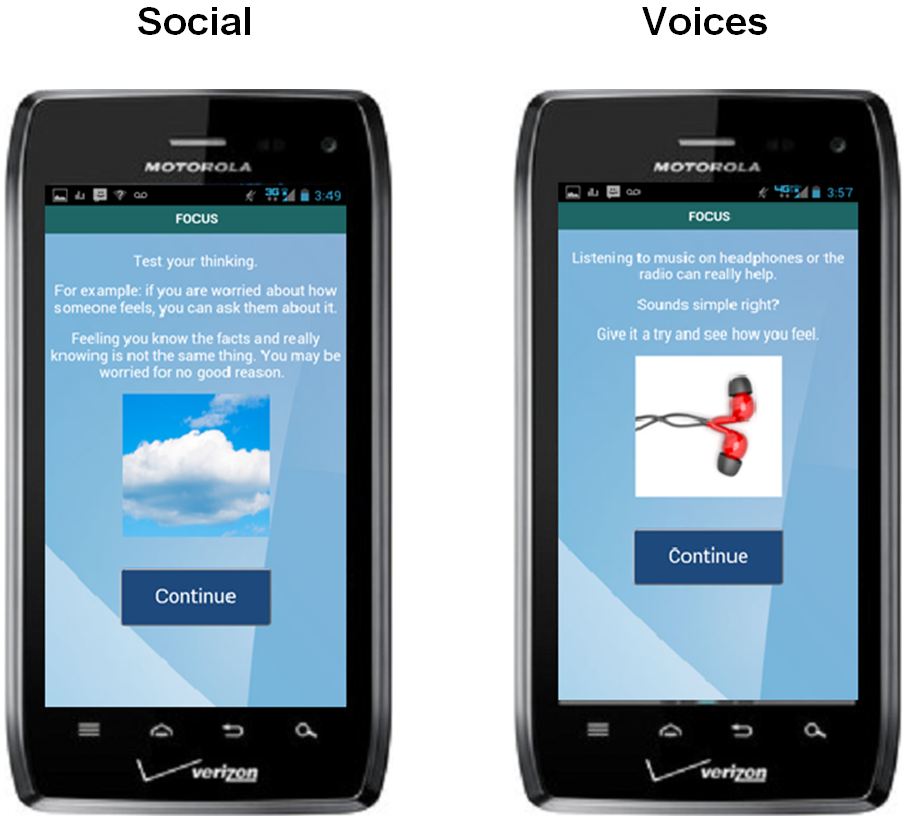

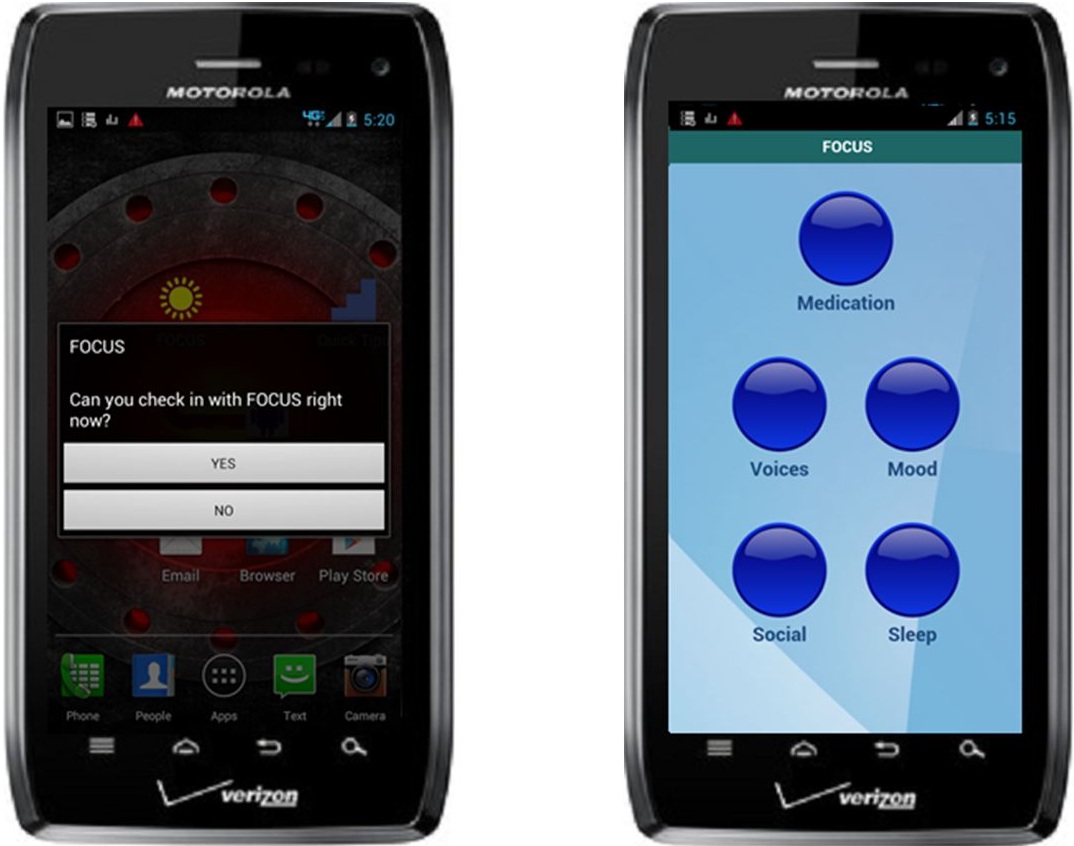
Targeting symptoms of psychosis was a complex challenge. Ben-Zeev distilled the software content, which can be downloaded onto Android smartphones, into brief interactive exchanges that are accompanied by illustrative images—photographs, cartoons, touchscreen reminder buttons—displayed on the smartphone screen. The easy to use system is both self-initiated and guided by prompts. For example, a FOCUS prompt will take over your smartphone screen and asks whether or not you can engage with the system. “If you say ‘yes’ it will launch the intervention scheduled for that time,” Ben-Zeev says.
Even patients with significant cognitive impairments, negative symptoms, or low literacy levels are able to use the app with ease and find the intervention helpful in managing their psychotic symptoms and depression.
Early feedback from testing the applications, indicates patients prefer to initiate interventions, rather than respond to prompts, and during the first two weeks of intervention, patients were using the system up to seven times per day. Interventions range from one to five minutes in duration—the high frequency, but low intensity, gives people an arsenal of quick tools to use whenever they are having a problem.
When used in harmony with face-to-face services, Ben-Zeev says, patients can use the mHealth interventions to enhance the therapeutic work they are already doing with their clinician. “There are a lot of contextual variables at work in a clinic setting,” he says. “Sitting across from someone in a white coat might impact the doctor-patient relationship—people may minimize their symptoms because they might not want the diagnosis or medications.” With the smartphone system, there is a sense of self-agency, it’s just you and the system; you elect how and when you want to use it.
Ben-Zeev’s intent is not to replace clinicians with technology. His motivation is the well being of patients. “FOCUS is giving us a level of information that exceeds anything we’ve had up until now. To my knowledge, this is the first smartphone intervention developed for schizophrenia,” he says. “If services and outcomes were optimal to begin with, there wouldn’t be the need for something like this.”
Think about it, Ben-Zeev says, “We have developed a treatment model for self-management that’s user-friendly, intuitive, and engaging. What’s not to like about that?”